
 Click image to enlarge
Click image to enlargehttp://farm4.static.flickr.com/3328/3498274531_2612922799_o.jpg
{kind=link}
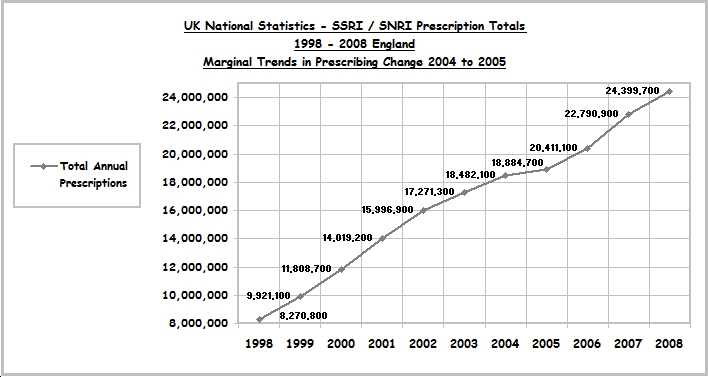
The obvious marginal trend change in Total Prescriptions 2004 to 2006 correlates with: -
1 The “Report of the CSM Expert Working Group on the Safety of Selective Serotonin Reuptake Inhibitors (SSRIs)” published December 2004 – which found the drug class lacking in safety and efficacy, not notably better than placebo.
http://www.mhra.gov.uk/home/groups/pl-p/documents/drugsafetymessage/con019472.pdf
2 The "House of Commons, Health Committee’s examination into The Influence of the Pharmaceutical Industry" - initiated June 2004 - report published April 5th 2005.
http://www.publications.parliament.uk/pa/cm200405/cmselect/cmhealth/42/42.pdf
3 “NICE Clinical Guidelines 23: Depression” published December 2004, issued new guidelines for treatment of depression with the introduction of the “Watchful waiting”; 1.4.1.2 a 2 week waiting period for patients with mild depression who did not want an intervention; and in 1.4.1.3 the GP to contact if the 2 week follow-up appointment not kept; and the restricting treatment initiation and management of Venlafaxine; 1.5.2.16 and in 1.5.2.17 to specialist mental health medical practitioners.
http://www.bpd-mind.fsnet.co.uk/NICE_Depression.pdf
The marginal trend change in Total Prescriptions 2004, caused the anomaly of a Total Prescription Increase of only 402.6 Thousand; the lowest annual SSRI / SNRI drug class increase in prescriptions in the 10 years available statistics.
Adjusting the median increases in SSRI / SNRIs total prescriptions 1998 to 2008 by removing year 2004 from the equation, increases the median total for 9 of the 10 years from over 1.61 Million per annum to over 1.74 Million.
****
Data collection reference:
Department of Health; NHS; Prescription Cost Analysis (PCA) - England.
1998 to 2007:
http://www.dh.gov.uk/en/PublicationsAndStatistics/Statistics/StatisticalWorkAreas/StatisticalHealthCare/DH_4086488
2008:
http://www.ic.nhs.uk/webfiles/publications/PCA%202008/PCA%202008.pdf
9–P-04 Tuesday
This comment has been removed by the author.
ReplyDeleteInteresting.
ReplyDeleteAre these figures for the whole of the UK or just England?
What point are you trying to make, it's unclear, unless of course, you are making claims that people who have suffered at the hands of Seroxat shouldn't have their day in court?
Is that your position?
It would also be credible if you added your full name to your work, that way you could at least stand by your convictions/opinions.
Why have you chose not to do this?
I consider your comment written in a tone anticipated to disturb, it’s clearly placed and intended – to a point – to be intimidating, threatening and confrontational, but I note you chose to delete your first comment; I’m not passing assumptions as to the contents, but if it was posted without thought – thank you for removing it!
ReplyDeleteAS I have stated quite clearly in the Blog, the statistics are collated from referenced verifiable government sources for England.
However, either way – as the UK population is approximately 60 million and England accounts for approximately 84% of that figure – the England Statistics used still encapsulate a sizable, wide and varied cross section of the UK population as a whole; in different geographical regions; being served by different NHS Trusts; encompassing age, health, nationality, ethnicity, race, religion, wealth, poverty, educational and employment status and both privileged and underprivileged areas; and I also add – will include a representation of both the Welsh and Scottish who reside in England.
I’m not sure what there is to be “unclear” about?
Although I did notice that you’ve commented at the bottom of the current page 'Marginal Trends in Prescribing Change 2004/05' – about half way through the Blog; rather than after the first inserted post 'Annual Prescriptions, Increases & Net Cost Variation Totals' or under the post 'Prescribing Trends Shift from Paroxetine 2001' - which I think is the post you’re commenting about?
I have made no claims, neither have I intimated or passed an opinion - on anything - the verifiable facts and statistics, stand alone, speak for themselves and are unbiased.
Whereas your question / statement - is a judgemental inference, based on conjecture, fabricated supposition and is biased.
When working with statistics a person does not have a “position” other than to be an objective instrument to interpret and report factual evidence in any other chosen medium.
The basic and chronologically referenced verifiable facts and statistic blogged will not differ how ever wide you make the catchment area.
If you interpret a correlation of irrefutable facts and statistics as an “Anti-Seroxat Litigation” statement – you have obviously missed the point completely!!
Along with the substantiation that the government appear to have used the “Report of the CSM Expert Working Group on the Safety of Selective Serotonin Reuptake Inhibitors (SSRIs)” published December 2004 and the "House of Commons, Health Committee’s examination into The Influence of the Pharmaceutical Industry" - initiated June 2004 - report published April 5th 2005, to facilitate the reduction of total net cost of the SSRI / SNRI drug class to it’s lowest point since 1998.
With regard the works credibility – all articles and documents are individually referenced to source, the Prescription Cost Analysis (PCA) Statistics are sourced from and referenced to the dh.gov.uk/en/PublicationsAndStatistics web site; the name the work is posted under is irrelevant to the creditability of the articles, documents and statistics.
I have posted on the drug boards as Tuesday, ID Tuesday1st, for over 7 years, during which time my stance, conviction and opinions have not changed; as you are the only person to ever question my use of name – I see no reason why that should change and it’s my prerogative to maintain that.
Also - just to clarify (having read your review) another of your disingenuous intentional misconception - there are NO comparisons of SSRI / SNRI side effects, withdrawal and ADRs in the Tuesday1st Blog.
Because there are NO statistics about SSRI / SNRI side effect, withdrawal or ADRs published in the UK Government Prescription Cost Analysis (PCA) Statistics on which the work is based.
And why the Blog is Called Tuesday1st UK: SSRI / SNRI Antidepressant Statistical Politics
And you are?
ReplyDeleteNot going to be bullied by you!
ReplyDeleteAfter all - aren’t you the one who advised another female poster on your own Blog - that one should “out” bullies?
“,that's enough for me.
Cynders.
5:33 PM
BOB FIDDAMAN said...
One would then assume Cynders that you would befriend someone you witnessed bullying a woman?
I have no gripe with you, I do notice how you tend to keep out of things on UK Survivors. Sometimes though Cynders, it pays to 'out' bullies and perverts because the longer they continue to get away with what it is they do, the more vulnerable innocents become.
Thanks for your input, on here at least.
5:38 PM
https://www.blogger.com/comment.g?blogID=10459981&postID=2158194675154537793
Posted by Fiddy at 15:24 0 comments”
Does that include you? Because being a bully is the impression you’re giving here?
It’s also very Machiavellian to play on another persons own, openly voiced concerns and vulnerabilities to try and assuage your own intentions!
You previously wrote to me twice on Jan 13th 09 - privately - choosing to reply to one of my posts to you on UKSurvivors (http://groups.yahoo.com/group/uksurvivors/message/41518) by email; I chose not to reply because I didn’t see why board issues should and could not be discussed on the open board where they were posted - I respected your privacy and that email has not been openly published.
So I’ll apologise now for breaking that confidence by quoting the following; “I wanted to create awareness on a bigger scale Tuesday, I felt that groups could not achieve this, hence the blog.“ ?
But apparently -- as your actions regarding this Blog have proved – your opinion is that other people are not allowed to create a bigger awareness of a very large issue, unless they restrict their efforts to and only support the ‘very small’ and ‘singled out part’ - that you think is important … and do so on your terms!!
Just because –
someone posts and advises you of irrefutable information that - if you gave some proper consideration and thought too, ‘could’ be beneficial to you and your cause – and all people affected by all drugs in the SSRI SNRI class because it’s posted in neutrality
and not under your “I hate Seroxat and GSK, lets Litigate” banner –
doesn’t make that work less viable, constructive or credible, neither does it automatically make that person the - enemy to be discredited, vilified and intimidated!
Your view that anyone who isn’t “with me” ---definition - specifically ranting against Seroxat and GSK--- is “against me” ---definition - a threat – and therefore a target--- is entrenched in nearly 7 years history of the UK Seroxat User Groups and Seroxat Campaign, you exported it to other groups (http://groups.yahoo.com/group/uksurvivors/message/18701) and have imported it to the blogs.
By coming here with deliberate intent to disrupt and undermine both the blogs content and me – you forced my hand to defend and explain that you had deliberately misrepresented what I had posted.
This Blog is not about any designated drug, it is neutral and reflects the stance I have taken on the drug boards for over 7 years; it encompasses all SSRI / SNRIs, focusing on their statistics, the politics, finances and prescribing trends; and will hopefully evolve to publish further information on regulatory policies, drug efficacy, patient safety and findings as they become available.
If you have genuine comments or questions that are pertinent to the Blogs contents you’re welcome to post here, but insofar as you’re current querulous and confrontational line of posting – it can remain here, but I’ll decline to respond and uphold the right to delete similar additional posts as I see fit.
Quote: -
”.......all you do is keep saying the person is out to sabotage the litigation – if there is no substance to what they are writing and a valid rock solid case - how can they?”
http://groups.yahoo.com/group/uksurvivors/message/41429 Sun Jan 11, 2009 1:02 pm
And your real name is?
ReplyDeleteCan you please guide me to find info about SSRI prescription for children and adolescents in the uk?
ReplyDeleteThanks